Healthy ageing
The NHS currently faces the unprecedented challenge of saving £20 billion by the year 2015. Approaches to achieving this goal can be broadly divided into two areas: ways to provide healthcare more efficiently and ways to reduce the demand for healthcare.
Historically it is the former that has been the main focus of discussions. Issues such as administrative structure, the funding of hospital facilities and the productivity of staff have dominated the agenda. Despite great effort by successive governments it has become clear that solutions tailored to tackling these issues can only take us so far. A more comprehensive answer to the problem requires us to focus less on continuous reform and to consider the demand placed on healthcare systems.
The reasons for increased cost are controversial. A classic argument attributes much of the increased cost to the increasing average age of the population. Although evidence suggests that age is only one driver of costs along with other factors like the greater use of expensive technology and pharmaceuticals1, age is undeniably a risk factor for many illnesses. As the greatest healthcare costs in a person’s life are spent around the time of death, regardless of how late that occurs, it is important to consider this issue in greater detail.
The driving forces for the shift in demographic distribution are largely similar worldwide: increases in life expectancy and declines in fertility. With age being a key risk factor for many pathologies, the number of people living with one or more chronic diseases is increasing, and hence also those requiring high cost healthcare. All this leads us to an important question: How do we enable people to remain free from the chronic diseases associated with ageing for as long as possible?
Over 30 years ago James Fries, an American academic and rheumatologist, wrote a seminal paper that helps us to answer this question. He made two observations:
1. The maximum human lifespan is fixed.
Even without the onset of specific diseases, the gradual decline in physiological and cellular reserves must lead to a ‘natural’ death in all people. In England and Wales, changes in the shape of the survival curve (below) with each passing decade show the age at death being pushed back over time and a steeper decline in survival as a maximum average lifespan is gradually approached.
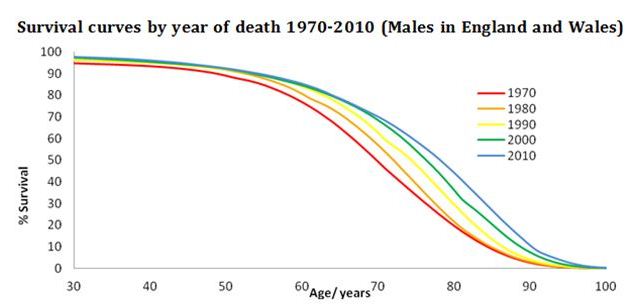
Adapted from data from the Office for National Statistics licensed under the Open Government Licence v.1.0. (Reproduced with permission).
2. The age of onset of chronic disease can be postponed.
At the time that Fries made this proposal, little data was available on morbidity in real populations. Since then numerous longitudinal studies, surveys and randomised trials have now confirmed that postponing morbidity is possible. Healthy behaviour has been shown to postpone morbidity more effectively than it postpones mortality3-7.
What follows from these two observations is that if we can postpone the onset of symptomatic disease then a reduction of overall morbidity is possible. This would allow people to live for longer without pain or disability and, importantly for the financial sustainability of healthcare systems, without the need for high-cost care.
Modern medicine and public health have often been called victims of their own success. Much of what is written about our ageing society is with an air of pessimistic resignation that the future holds only infinite infirmity and impossible healthcare costs. A concerted approach focussing on preventative healthcare would remove the need for such despair. Society could then look forward to fewer years of ill health and healthcare workers could take pride in their role in helping to achieve this.
Rahul Bahl, FMLM Medical Student Group, UCL Medical School.
References:
- Appleby J. Spending on health and social care over the next 50 years Why think long term? London: The King's Fund, 2013.
- Fries JF. Aging, natural death, and the compression of morbidity. N Engl J Med 1980;303(3):130-5.
- Hubert HB, Fries JF. Predictors of physical disability after age 50: Six-year longitudinal study in a runners club and a university population. Ann Epidemiol 1994;4(4):285-94.
- Vita AJ, Terry RB, Hubert HB, Fries JF. Aging, health risks, and cumulative disability. N Engl J Med 1998;338(15):1035-41.
- Chakravarty EF, Hubert HB, Lingala VB, Fries JF. Reduced disability and mortality among aging runners: A 21-year longitudinal study. Arch Intern Med 2008;168(15):1638-46.
- Chakravarty EF, Hubert HB, Lingala VB, Zatarain E, Fries JF. Long distance running and knee osteoarthritis: A prospective study. Am J Prev Med 2008;35(2):133-8.
- Fries JF, Bruce B, Chakravarty E. Compression of morbidity 1980-2011: a focused review of paradigms and progress. J Aging Res 2011;2011:261702.