Never Events
The importance of protecting patients from avoidable harm is self-evident. No more so than when there are clearly defined processes and procedures available to help ensure that incidents such as never events simply do not happen. Yet despite such processes and procedures some of the never events listed in the National Policy Framework[1] have happened, and continue to occur. We must, therefore, work together to improve patient safety.
Never events are serious, preventable patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare providers[1]. Incidents are conisdered to be never events if they meet the following criteria:
The incident either did result in actual severe harm or death or had the potential to lead to severe harm or death[2].
- There is evidence that the never event has occurred in the past and that it is a known source of risk (for example through reports to the National Reporting and Learning Service or other serious incident reporting system)
- There is existing national guidance and/or national safety recommendations on how the event can be prevented as well as support for implementation of the relevant preventative measures
- The event is preventable if national guidance and/or national safety recommendations are implemented
- Occurrence of the never event can be easily identified, defined and measured on an ongoing basis
There are 25 classifications of never events specified in NHS England (see section 8 National Patient Safety Agency, ‘Never Events – Framework: Update for 2010-11’). This list was developed in 2011 from an original list of eight never events as defined by the NPSA in 2009.
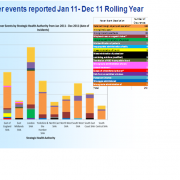
The never events list provides a lever for those in the NHS to improve patient safety through greater focus, scrutiny, transparency and accountability when very serious patient safety incidents occur. The existence of the never events list should therefore, be seen as a key driver in ensuring unrelenting focus on the eradication of these preventable and extremely serious incidents. Yet despite this, patients continue to be harmed. Table one below illustrates the never event profile for England this year.
Table one:
The occurence of a never event could be viewed as an indication that an organisation has not put in place the right systems and processes to prevent the incidents from happening and thereby prevent harmful outcomes. The occurrence and reporting of them is also an indicator of how safe an organisation is. However, the list does not exist to allow greater blame or punishment to be levelled on individuals. In fact the principle of a never events list only works where organisations establish an open safety culture and a just blame culture.
This means:
‘’…staff within an organisation have a constant and active awareness of the potential for things to go wrong. Both the staff and the organisation are able to acknowledge mistakes, learn from them, and take action to put things right. Being open and fair means sharing information openly and freely and fair treatment for staff when an incident happens.
…the causes of a patient safety incident cannot simply be linked to the actions of the individual healthcare staff involved. All incidents are also linked to the system in which the individuals were working. Looking at what was wrong in the system helps organisations to learn lessons that can prevent the incident recurring.’’ [3]
It is possible for never events to be the result of poor practice by an individual rather than the system in which they work. These instances are rare, but the incident Decision Tree developed by the NPSA can help managers and senior clinicians determine if it is appropriate to take action concerning an individual practitioner. [4]
Reporting is the first stage in learning the lessons from an incident and ensuring it can never happen again. Failure to report is simply unacceptable and a sign of real cultural and safety failings in an organisation. As has been noted by Sir Liam Donaldson, "to err is human, to cover up is unforgivable, and to fail to learn is inexcusable".
Ultimately it does not matter whether an incident matches a never events definition; patients must be protected from avoidable harm. Driving the incidence of never events to zero requires the concerted effort and focus of all those working in the NHS. While the policy framework can be set nationally, it is those providing care who are accountable for the services they deliver. From ward to board, all sections of an organisation must play their part but more importantly perhaps, is for senior doctors responsible for upholding high standards of clinical practice to lead by example and work to eradicate never events.
[1] National Patient Safety Agency, ‘Seven Steps to Patient Safety’’, 2004 – 2009. Available at www.nrls.npsa.nhs.uk/resources/collections/seven-steps-to-patient-safety/
[2] National Patient Safety Agency ‘Incident Decision Tree’ 2004. Available at www.nrls.npsa.nhs.uk/resources/?EntryId45=59900
[3] National Patient Safety Agency, ‘Never Events – Framework: Update for 2010-11’, March 2010. Available at www.nrls.npsa.nhs.uk/resources/?entryid45=68518
[4] For some types of never event, there does not have to have been actual severe harm or death for the incident to be classed as a never event. The never events criteria require that the type of incident has the potential to cause severe harm or death. For some never events, an incident in which neither severe harm or death results is still a never event, for example wrong site surgery. For other types of never event, severe harm or death must result for the incident to be classed as a never event, for example maladministration of insulin.